CEREBRAL ANEURYSM – Overview and Treatments
Introduction
Cerebral Aneurysm has always been labelled as silent killer, hiding in the brain without indications. No obvious symptoms but can kill patients in a second. Most of the time, the cerebral aneurysm was only revealed at the time it ruptured, leading to an acute stroke or severe headache for patients.
Aneurysms can appear anywhere in arteries, but most commonly are at the cerebral arteries and aorta. Common cerebral hemangioma sites include the anterior cerebral artery(30-35%), internal carotid artery and posterior cerebral artery (30-35%), middle cerebral artery (20%), basilar artery and posterior cerebral artery.
Rupture of aneurysm has a huge impact on social medical resources, economic burden on patients’ family members, and also physical and mental disability of patients. If preventive treatment can be received by patients before the aneurysm ruptured, tragedies can be avoided. This Overview and Treatments provides some basic knowledge about cerebral aneurysms and answers to some frequently asked questions for patients and their families.
What is Cerebral Aneurysm?
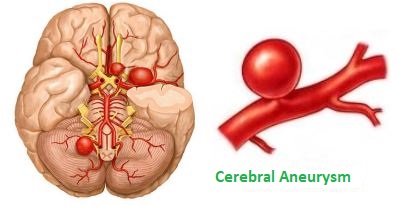
A cerebral aneurysm is a ballooning arising from a weakened area in the wall of a blood vessel in the brain. It often looks like a berry hanging on a stem.
How does Cerebral Aneurysm form?
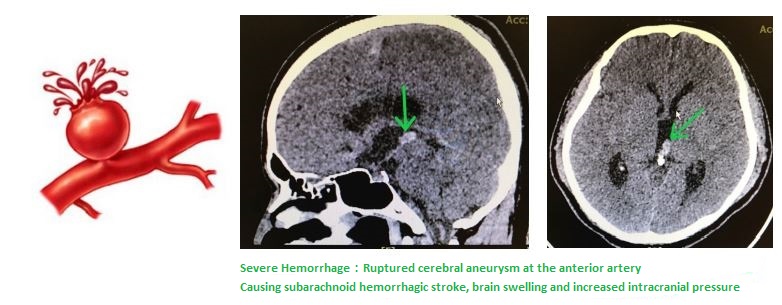
Cerebral aneurysm is a cerebrovascular disease. Aneurysms develop as a result of thinning artery walls. Aneurysms often form at forks or branches in arteries because those areas of the vessels are weaker. When the cerebral aneurysm expands and the blood vessel wall becomes too thin, the aneurysm will rupture and bleed into the space around the brain. This event is called a subarachnoid hemorrhage (SAH) and may cause a hemorrhagic (bleeding) stroke, mortality rate of which could be up to 36%.
The presence of a cerebral aneurysm may not be known until it ruptures. Aneurysms in children is appeared to be less likely to occur. They are most common in adults between the ages of 30 and 60 and are more common in women than in men. People with certain inherited disorders are also at higher risk. Inherited arterial wall weakness may be a factor in aneurysms. Occasionally, severe head injuries or infection may lead to the formation of aneurysm.
In Hong Kong, there are about 5 cases for every 100,000 people, mainly middle-aged. The male to female ratio is 1 : 2. Smoking, high blood pressure, injuries or cerebral artery injuries are more commonly causes of cerebral aneurysm
What are the Symptoms of Cerebral Aneurysm?
Most cerebral aneurysms do not show symptoms until they either become very large or rupture. Small unchanging aneurysms generally will not produce symptoms and mostly were only revealed after physical examinations. Occasionally, there may be symptoms that happen before a rupture due to a small amount of blood that may leak. This is called “sentinel hemorrhage” into the brain. Some aneurysms are symptomatic because they gradually grows in size and press on adjacent structures, such as nerves to the eye. They can cause visual change/loss or diminished eye movements, even if the aneurysm has not ruptured.
A ruptured aneurysm quickly becomes life-threatening and requires prompt medical
treatment. 20-30% patients died before they were sent to the hospital. If the ruptured cerebral aneurysm is not treated in time, 40% of those will rupture again in the following six months, and the mortality rate will be increased to 70%
Ruptured Cerebral Aneurysm
Aneurysms may rupture and bleed into the space between the skull and the brain
(subarachnoid hemorrhage) and sometimes into the brain tissue (intracerebral hemorrhage). These are forms of stroke called hemorrhagic stroke. The bleeding into the brain can cause a wide spectrum of symptoms, from a mild headache to permanent damage to the brain, or even death.
In addition to a severe headache, common signs and symptoms of a ruptured aneurysm include nausea and vomiting, stiff neck, blurred or double vision, sensitivity to light, a drooping eyelid or loss of consciousness.
After an aneurysm has ruptured it may cause serious complications such as:
Rebleeding – Once it has ruptured, an aneurysm may rupture again before it is treated, leading to further bleeding into the brain, and causing more damage or death. Change in sodium level – Bleeding in the brain can disrupt the balance of sodium in the blood supply and cause swelling in brain cells. This can result in permanent brain damage.
Hydrocephalus – Subarachnoid hemorrhage can cause hydrocephalus. Hydrocephalus is a buildup of too much cerebrospinal fluid in the brain, which causes pressure that can lead to permanent brain damage or death. Hydrocephalus occurs frequently after subarachnoid hemorrhage because the blood blocks the normal flow of cerebrospinal fluid. If left untreated, increased pressure inside the head can cause coma or death.
Vasospasm – This occurs frequently after subarachnoid hemorrhage when the bleeding causes the arteries in the brain to contract and limit blood flow to vital areas of the brain. This can cause strokes from lack of adequate blood flow to parts of the brain.
Seizures – Aneurysm bleeding can cause seizures (convulsions), either at the time of bleed or in the immediate aftermath. While most seizures are evident, on occasion they may only be seen by sophisticated brain testing. Untreated seizures or those that do not respond to treatment can cause brain damage.
Unruptured Cerebral Aneurysm
An unruptured cerebral aneurysm may produce no symptoms, particularly if it’s small. It may only be revealed until physical examination. For larger unruptured aneurysm, it may press on brain tissues and nerves, possibly causing:
- pain above and behind one eye
- drooping eyelid
- change in vision or double vision
- numbness of one side of the face
Headache is not common for unruptured cerebral aneurysm. Rare case for unruptured aneurysm along with ruptured aneurysms, possibility of 20% among patients. Treatment for unruptured aneurysm may prevent a rupture in future.
How the Cerebral Aneurysm is diagnosed?
When there is a suspecting ruptured aneurysm, a Computed Tomography (CT) can be used to detect intracranial hemorrhage. The disadvantage is that the cause of the hemorrhage cannot be clearly indicated. After injecting with a contrast dye into patient’s bloodstream, the aneurysm can be visualized through a special imaging technique called Computed Tomography Angiography (CTA), which produces sharper, more detailed images of blood flow in the brain arteries. CTA can show the size, location, and shape of an unruptured or a ruptured aneurysm.
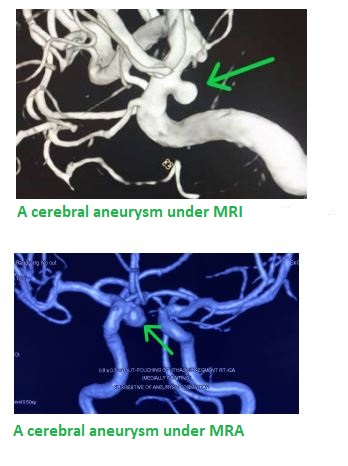
Magnetic Resonance Imaging (MRI) uses computer-generated radio waves and a magnetic field to create two- and three-dimensional detailed images of the brain and can determine if there has been bleeding into the brain. Magnetic Resonance Angiography (MRA) produces detailed images of the brain arteries and can show the size, location, and shape of an aneurysm. MRI is a technology of radiation-free, harmless and painless, which is totally different from the radiative X-ray Scan. No contrast dye is required during examination.
MRI can be used to screen different parts of the body, including a whole-body MRI examination for asymptomatic patient to detect signs of potential stroke or cancer.
Treatments
Current treatment options:
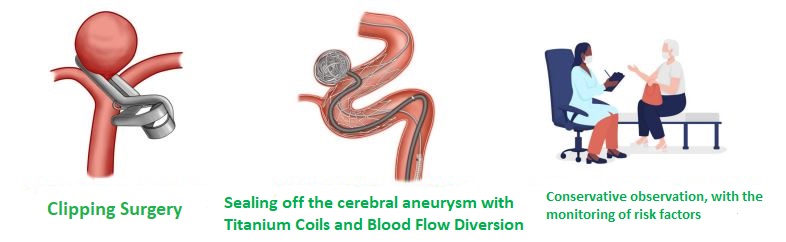
- Microvascular Clipping(Clipping Surgery);
This procedure involves cutting off the flow of blood to the aneurysm and requires open brain surgery. The neurosurgeon will locate the blood vessels that feed the aneurysm and place a tiny, metal, clothespin-like clip on the aneurysm’s neck to stop its blood supply. With this, the risk of aneurysm rupture to cause severe bleeding stroke, brain damage or even death will be eliminated. - Endovascular Neurovascular Surgery (to seal off the cerebral aneurysm with Titanium Coils and Blood Flow Diversion Stent);or
Just a 1-hour Minimally Invasive Procedure via a needle puncture and with using a fine catheter, in order to seal off and to obliterate the aneurysm, so as to deactivate the bomb inside brain.Under X-ray control as road-mapping guidance, via a needle puncture wound to the femoral artery at patient’s groin with using a hair-pin like, extremely fine microcatheter, Neurovascular Surgeons will navigate to patient’s brain vessels, aiming at deploying a Titanium Blood Flow Diversion Stent across the neck of the aneurysm, so as to block the blood from inflowing into the aneurysm sac. Successful aneurysm obliteration will result in shrinking the aneurysm with time.At the same time, for big aneurysm, Neurovascular Surgeons may also implant
Titanium Coils inside the aneurysm sac so as to enhance the blockage of blood inflow.Overall, the surgical aim is to exclude the aneurysm from the blood flow, and to strengthen the wall of blood vessel at brain. Thus, the risk of aneurysm rupture to cause severe bleeding stroke, brain damage or even death will be eliminate
- Conservative observation, with the monitoring of risk factors
According to the condition and needs of the patient after the examination and
imaging investigation, patients who choose not to have surgery should take
medication on time, control their diet, and have regular MRI at brain to review and monitor the status. However, if the risk factors are out of control, ever for a 1mm cerebral aneurysm, may cause to death in case of aneurysm rupture (mortality rate up to 36%). Therefore, this treatment option is the least suggested.
Comparison on Different Treatment Options
| Pros | Cons/Risk | |
| Microvascular Clipping(Clipping Surgery) |
|
|
| Endovascular Neurovascular Surgery(to seal off the cerebral aneurysm with Titanium Coils and Blood Flow Diversion Stent) |
|
|
| Conservative Observation |
|
|
Factors to be Considered in Making Decision on Treatment Options
Neurological status, underlying disease, age, location, size, and shape of the aneurysm, risk of aneurysm rupture, existing treatment conditions, and nature of the aneurysm (ruptured vs. unruptured) are the factors to consider in making treatment decisions. The doctor will analyze and propose the most suitable treatment for the patient based on the above factors.
For example, aneurysms located on the dorsal side of the brain are more safely embolized with titanium coils. For elderly or critically ill patients, endovascular intervention is more advantageous because it does not require prolonged deep anesthesia. Open surgery is a good option for healthy young adults because of the better long-term result with clipping. In general, doctors will propose the treatment option with the lowest risk and the highest success rate for the patient.
The purpose of treatment is to prevent bleeding or rebleeding of the affected area caused by rupture of the aneurysm. Once an aneurysm ruptures and bleeds, there is a high risk of rupturing again, especially within 48-72 hours after the first bleed, and each bleed reduces the patient’s chances of recovery.
When making the decision on the way to treat an unruptured aneurysm, there is usually a trade-off of risk, and it varies from each patient. Below are some of the factors to be considered:-
- big aneurysms at certain specified locations are considered as more likely to rupture;
- aneurysm at specified location are considered as more likely to rupture
- patients with aneurysms bleeding at earlier stage are at greater risk of aneurysm rupture;
- patients with family history of aneurysms are at greater risk of aneurysm rupture.

Points to Note Before & After Surgery
Before-Surgery:
- The neurosurgeon will explain the purpose and procedure to the patient and his/her family according to the location of the aneurysm, and the patient or his/her family will be requested to complete the Consent for Surgery, Consent for Anesthesia, Confirmation on Surgery Fee and Disbursements, Consent for Blood Transfusion, and Consent for Intensive Care Unit (if applicable)
- Examinations before surgery include: Electrocardiogram (ECG), chest X-Ray, blood test, angiography, etc.
- Skin preparation: Some hair on the surgical site may need to be shaved.
- General anesthesia will be adopted for the surgery.
- Patient should follow doctor’s instructions to take his/her own chronic disease medication, such as medication for blood pressure. If patient is taking anticoagulant (a drug that prolongs blood clotting time and reduces blood clotting), patient should take initiative to inform doctor in advance, and withhold the drug intake according to doctor’s instructions before surgery to avoid bleeding.
*Please note:If patients are uncertain whether the medications they are receiving contains anticoagulants, please let your doctor know and provide the name of the drugs. - No eating or drinking after midnight (12:00 am), the night before surgery.
- Patients need to change the surgical clothing and take off the underwear, glasses (including contact lenses), dentures, nail polish, and body accessories on the day of surgery
After-Surgery:
- Patient will be sent to the intensive care unit after the surgery. Subject to patient’s stable breathing conditions, the endotracheal tube can remove, as decided by the doctor.
- Keep the limb on the puncture side as straight as possible
- Patients must stay in bed for 6 hours after the surgery, during which the medical staff may assist patients to turn over, according to patients’ condition.
- Consent from doctor is required before get out of bed.
- After patients’ condition become stable, if no further changes, patients can be discharged from hospital after one day or two, with the consent of doctor.
- Please maintain smooth defecation and do not force defecation. Medication will be given by doctor when necessary, and patients are also advised to have more
vegetables and fruits. - Patients should keep their blood pressure stable. If patients are taking blood pressure drugs, anti-vasospasm (nimodipine), etc., please follow doctor’s instructions and do not stop the drug intake on your own decision. In case of obvious headache, patients should consult doctor immediately.
- If the aneurysm was ruptured and bled previously, there may be sequelae of hydrocephalus. If drowsiness or limb weakness occurs, please consult doctor immediately.
Risks and Complications
The risks and complications of minimally invasive surgery are basically similar to those of traditional clipping surgery. Patient’s condition, size and location of aneurysm, all are the factors that determine surgical risk. The surgical risk of ruptured aneurysms is approximately 10% to 20% while risk of rupture can be high as 30% for larger aneurysms growing deep inside the brain. A hemorrhagic (bleeding) or ischemic stroke can be occurred few days after the aneurysm was treated. Risk of anesthesia is usually in relation to age and heart, lung, liver and kidney functions, and an anesthesiologist will usually be consulted before surgery.
The risks of surgery itself include bleeding, infection, and nerve damage. Another surgery to remove blood clot or decompression may be required in case of rebleeding or severe ischemic stroke after the surgery. Mild infections are usually treated with antibiotics, but severe infections (e.g. brain abscesses) may require surgery. Basically, the probability of requiring another surgery is less than 8-15%, and most of them are due to hydrocephalus and need to place a ventriculoperitoneal drainage device. Due to the lower brain damage for Endovascular Neurovascular Surgery, the proportion of nerve damage is also lower than that of traditional craniotomy. Any neurosurgery may have the risk of death, paralysis or persistent vegetative state. However, surgical risk can be significantly reduced if the surgery is performed by an Endovascular Neurovascular Neurosurgeon who is experienced and licensed to operate digital subtraction angiography equipment for endovascular treatments.
Other surgical risks and complications include the followings:
- If the blood vessel is accidentally punctured, it may result in local hematoma, blood vessel damage, terminal necrosis, etc
- Possible risk and factors that cannot be prevented in this surgery, which may lead to the deterioration of the condition:
- deterioration in condition of the disease itself, such as sudden rupture of aneurysm and rebleeding;
- during the surgery while the extremely fine micro-catheter is being navigated inside patient’s brain, the cerebral blood vessels may rupture, and even lead to death in severe cases.
- implantation of titanium coils for embolization or after embolization may block nearby normal blood vessels, or cause stroke due to coil displacement.
- cerebral vasoconstriction causing ischemic stroke.
- neurological complications: permanent or temporary loss of nerves, subarachnoid hemorrhage and bleeding stroke.
- segmental laceration of intracranial blood vessels, vascular embolism.
- adverse reactions and other drug allergies after injection of iodine-containing
contrast dye.
How are Neurovascular Neurosurgeons
performing a Minimally Invasive
Endovascular Neurosurgery in Implanting a
Blood Flow Diversion Stent for Obliterating
a Cerebral Aneurysm
Disclaimer
The content of this Introduction and Treatment Overview is for general and reference purposes only. It aim to enable patients and their families to have a basic understanding of the disease and different treatment options before deciding to receive treatment. Patients need to make their own treatment decisions based on their actual conditions. This Overview does not provide a diagnosis or recommended treatment for any individual patients. Any treatment plan has its potential risks and hence patients must cooperate with medical staffs and doctors.

